")

Speech and non-speech motor control of the oral-laryngeal-respiratory system: clinical studies
Dr. Anja Staiger & Prof. Dr. Wolfram Ziegler
Contact: anja.staiger@ekn-muenchen.de
Clinical partners:
- Department of General Neurology, Hertie Institute for Clinical Brain Research, University of Tübingen, Prof. Dr. H. Ackermann, Dr. Bettina Brendel & Prof. Dr. L. Schöls
- Interdisciplinary outpatient department for atypical Parkinsonian disorders, Department of Neurology, Klinikum der Universität München, Ludwig-Maximillians-University Munich, Prof. Dr. med. S. Lorenzl
- Department of Neurology, Klinikum der Universität München, Ludwig-Maximillians-University Munich, Prof. Dr. med. K. Bötzel
Research assistants:
Verena Schneider, Stefanie Schmid
Several theories of speech motor control are implicitly based on the assumption that the neural control mechanisms subserving the generation of speech and non-speech movements of the oral-laryngeal-respiratory system (lips, tongue, jaw, velum, pharynx, larynx and the respiratory apparatus) are identical or at least overlapping. According to such a model, it should be expected that a disorder affecting one oral motor activity - such as speaking - necessarily affects all other motor activities alike (e.g., chewing, swallowing, emotional expression, volitional movements such as blowing, whistling or tongue protrusion). In fact, this assumption is reflected in several accounts on both, the pathomechanisms and the management of the dysarthrias. As an example, standard dysarthria assessment tools (e.g., Frenchay-Dysarthria-Assessment; Enderby & Palmer, 2008) typically include non-speech oral motor tasks in order to determine the profile and severity of dysarthria. Further, a number of well-established treatment methods at least partially rely on non-speech oral motor exercises in order to enhance speech performance (e.g., Mackenzie et al., 2010).
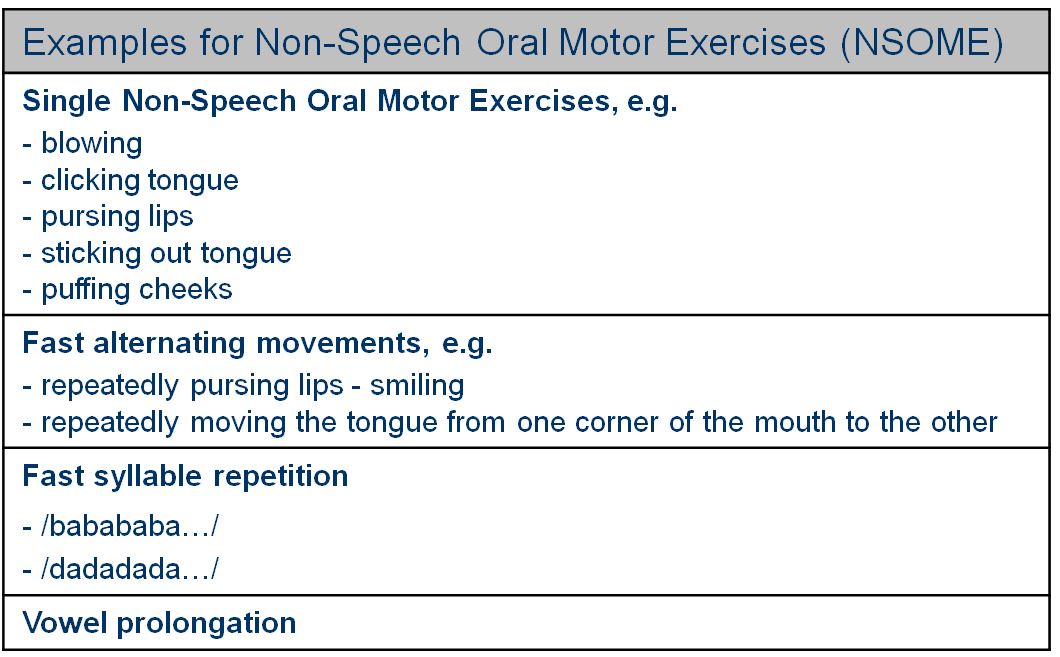
However, clinical dissociations (e.g., disordered speech but intact non-speech oral motor abilities) as well as further theoretical reasons argue for an involvement of distinct sensory-motor control systems in the generation of speech and non-speech movements and thus for a task-dependent organization of speech motor control processes (e.g., Ziegler, 2003).
With the current study we aim to contribute to this discussion using a clinical approach. The study comprises a large sample of neurologically impaired patients with different etiologies (e.g., Parkinson's disease, stroke, cerebellar diseases). Several speech and non-speech skills are examined in order to reveal performances and possible dissociations. The study thus sets the stage for a theoretically founded dysarthria assessment and treatment.
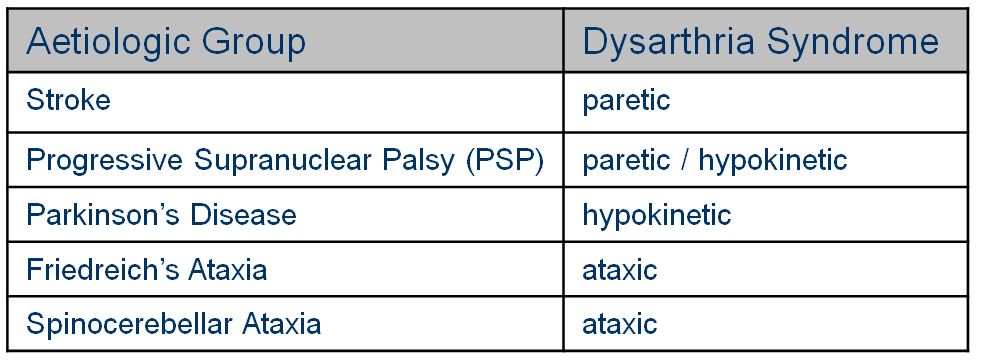
The etiologic groups participating in the study represent important clinical dysarthria syndromes (paretic, hypokinetic, ataxic) and their combinations. However, the presence of dysarthria is NOT a criterion for inclusion. This allows for a description of patients with intact speech abilities but possible deficits in non-speech oral motor tasks. As a control group we examine neurologically healthy, age-matched persons.
Project extension:
Within the scope of a PhD scholarship of the German National Academic Foundation (Studienstiftung des deutschen Volkes), Theresa Schölderle investigated a group of patients with cerebral palsy.
References:
- Enderby, P. M. & Palmer, R. (2008). Frenchay Dysarthria Assessment. (2nd ed.) Austin, TX: Pro-Ed.
- MacKenzie, C., Muir, M., & Allen, C. (2010). Non-speech oro-motor exercise use in acquired dysarthria management: regimes and rationales. International Journal of Language & Communication Disorders, 45, 617-629.
- Ziegler, W. (2003). Speech motor control is task-specific: evidence form dysarthria and apraxia of speech. Aphasiology, 17, 3-36.
 supported by the German Research Foundation (DFG) (ZI469 / 15-1/2)
supported by the German Research Foundation (DFG) (ZI469 / 15-1/2)